Ovarian cysts — fluid-filled sacs on or within the ovary — are extremely common and in the vast majority of cases represent normal physiological processes (functional cysts) rather than pathological conditions. Most ovarian cysts are asymptomatic and discovered incidentally on ultrasound performed for other reasons. Understanding which cysts require monitoring or treatment — and which can safely be observed — is an important component of women’s gynecological care. This guide explains how clinics evaluate and manage ovarian cysts.
Types of Ovarian Cysts
Functional Cysts
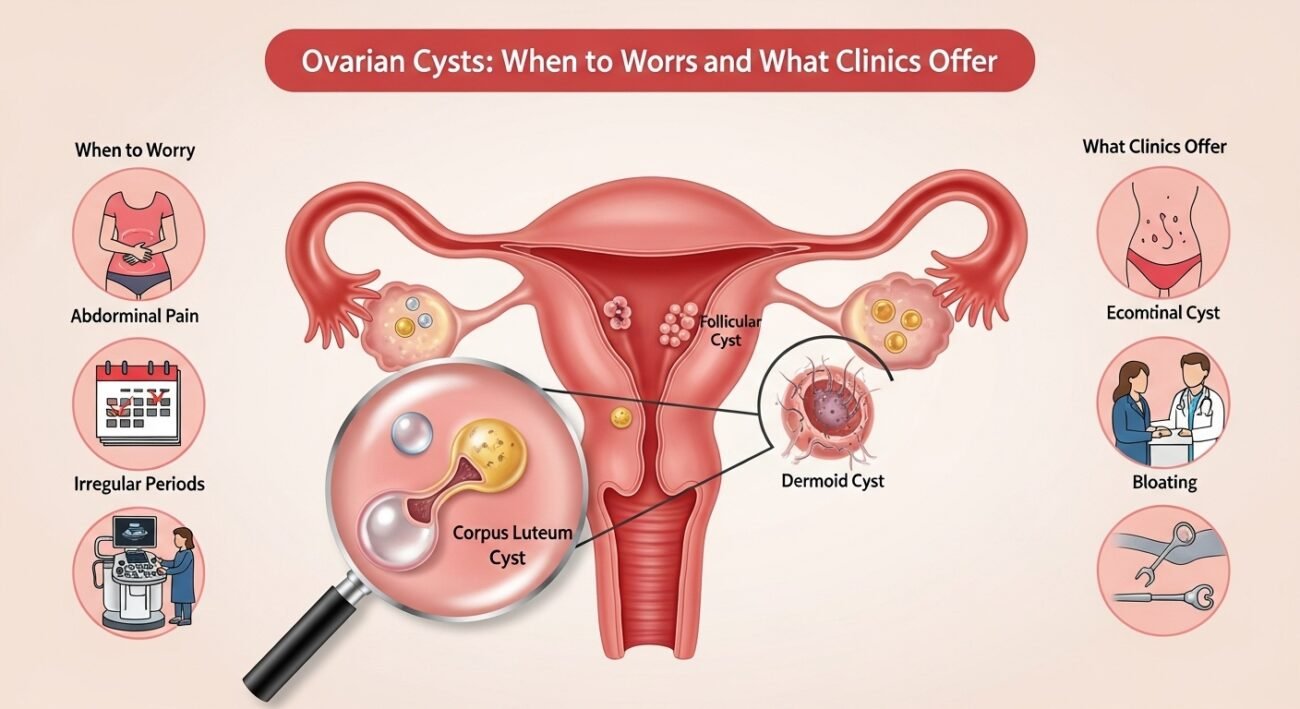
The most common type — follicular cysts (from follicles that didn’t release an egg) and corpus luteum cysts (from the follicle after egg release) develop normally during the menstrual cycle and almost always resolve spontaneously within 1–3 menstrual cycles. They are typically asymptomatic or mildly tender, less than 5 cm, and require no treatment beyond watchful waiting with repeat ultrasound.
Endometriomas
Ovarian cysts containing old menstrual blood (“chocolate cysts”) arising from endometriosis. Managed in the context of overall endometriosis treatment — surgical removal for large endometriomas before IVF is sometimes appropriate.
Dermoid Cysts (Mature Teratomas)
Containing tissues from other body parts (hair, skin, sometimes teeth) — benign but often require surgical removal due to size and torsion risk.
Cystadenomas
Benign epithelial cysts that can grow large — often require surgical evaluation when large or symptomatic.
Features Prompting Concern
Ovarian cyst features raising concern for malignancy include: postmenopausal status, solid components, internal blood flow on Doppler ultrasound, thick septations, large size (greater than 10 cm), bilateral cysts, and elevated CA-125 tumor marker. These features prompt specialist evaluation and careful surgical decision-making.
Ovarian Torsion
Ovarian torsion — twisting of the ovary on its vascular pedicle causing blood supply interruption — is a gynecological emergency presenting with sudden severe unilateral pelvic pain. It requires emergency surgical detorsion (unwinding the ovary) to preserve ovarian function.
Conclusion
The vast majority of ovarian cysts in reproductive-age women are benign functional cysts requiring only watchful observation. Those with concerning features warrant specialist evaluation. If you have been told you have an ovarian cyst, ask your gynecologist specifically what type it appears to be, what monitoring is planned, and what symptoms would require urgent evaluation.
FAQs – Ovarian Cysts
Q1. Do ovarian cysts cause pain?
A: Most ovarian cysts cause no symptoms. Large cysts may cause dull pelvic pressure. Rupture of a cyst can cause sudden sharp pain (typically resolving as the fluid is absorbed). Cyst torsion causes severe sudden pain requiring emergency care. Contact your clinic for any sudden, severe pelvic pain.
Q2. Can I get pregnant with an ovarian cyst?
A: Yes. Most functional ovarian cysts do not affect fertility. Endometriomas can impair fertility and may require treatment before attempting conception. Polycystic ovarian morphology (multiple small follicles associated with PCOS) is managed as part of PCOS treatment when fertility is affected.
Q3. How often are ovarian cysts cancerous?
A: The vast majority of ovarian cysts are benign — particularly in premenopausal women. Ovarian cancer risk from cysts increases with postmenopausal status, older age, complex cyst features, and elevated CA-125. Most cysts in reproductive-age women are not malignant.
Q4. Does the birth control pill help ovarian cysts?
A: Combined oral contraceptives suppress ovulation and prevent new functional cysts from forming — they are sometimes prescribed for women with recurrent functional cysts. They do not accelerate resolution of existing cysts. They do not treat endometriomas or other pathological cysts.
Q5. What is CA-125 and should I have it tested for an ovarian cyst?
A: CA-125 is a blood tumor marker elevated in ovarian cancer but also commonly elevated in benign conditions including endometriosis, fibroids, pregnancy, and pelvic inflammatory disease. It has poor specificity in premenopausal women. CA-125 is most useful when combined with ultrasound characteristics in postmenopausal women with complex cysts to assess malignancy risk.