Hip pain is an extremely common complaint in primary care and orthopedic clinics, with prevalence increasing with age. The hip is a deep ball-and-socket joint bearing enormous loads — and its proximity to major nerve structures (sciatic nerve), numerous bursae, and the lumbar spine creates a diagnostic challenge: pain perceived in the hip region may originate from the hip joint itself, the lumbar spine, the sacroiliac joint, or soft tissue structures around the hip. Accurate diagnosis is essential for effective treatment. This guide explains how clinics evaluate and manage hip pain and disorders.
Common Hip Conditions
Hip Osteoarthritis
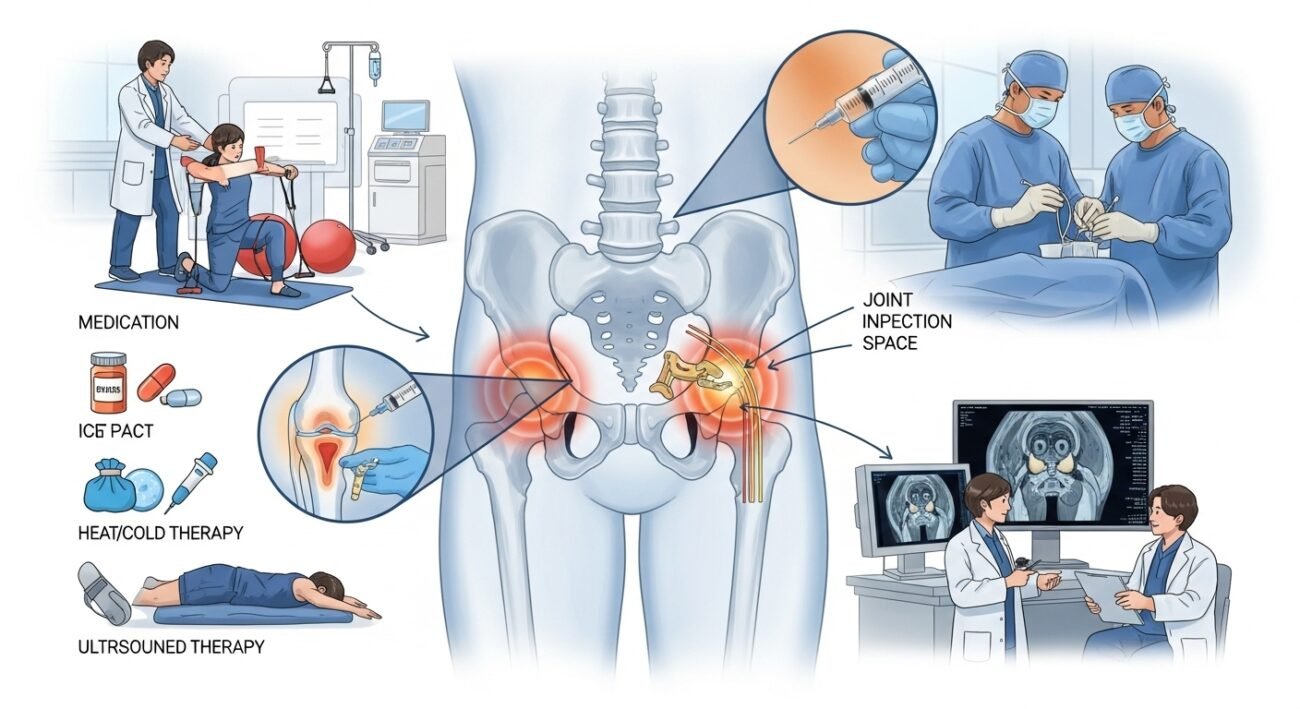
The most common cause of true hip joint pain in older adults — causing groin pain (the most reliable indicator of true hip joint pathology), limited range of motion, and a characteristic antalgic gait. Conservative management includes weight loss, physical therapy (hip and core strengthening), NSAIDs, corticosteroid injections, and ultimately total hip replacement for advanced disease with uncontrolled pain and functional limitation.
Greater Trochanteric Pain Syndrome (Trochanteric Bursitis)
Lateral hip pain over the greater trochanter — now understood to arise primarily from gluteal tendinopathy rather than true bursitis. Reproduced by direct lateral pressure, single-leg stance, and hip adduction. Treatment includes activity modification, physical therapy with gluteal tendon loading protocol, and corticosteroid injection for acute flares.
Hip Fractures
Femoral neck and intertrochanteric fractures are common in older adults with osteoporosis, caused by falls. They represent medical emergencies requiring surgical fixation or arthroplasty within 24–48 hours for optimal outcomes. Prevention through falls risk management and osteoporosis treatment is the most important clinical strategy.
Diagnostic Approach
Clinical examination distinguishes hip joint pathology (groin pain, restricted internal rotation) from soft tissue and referred pain sources. Plain X-rays assess joint space narrowing, fracture, and deformity. MRI provides superior evaluation of soft tissue, labral pathology, avascular necrosis, and stress fractures. CT clarifies complex bony anatomy for surgical planning.
Conclusion
Hip pain management begins with accurate diagnosis — determining whether pain originates from the hip joint, periarticular soft tissues, or referred from adjacent structures determines the most effective treatment pathway. Physical therapy is the cornerstone of non-operative hip pain management; surgical intervention is reserved for conditions that genuinely require structural repair or replacement for restoration of function.
FAQs – Hip Pain
Q1. What does hip joint pain feel like?
A: True hip joint pain (from the ball-and-socket joint) is typically felt in the groin, sometimes radiating down the front of the thigh. Pain felt on the outside of the hip (lateral hip pain) more commonly arises from periarticular structures (trochanteric bursitis, IT band). This distinction helps guide examination and imaging.
Q2. How long does recovery take after hip replacement?
A: Most patients are walking with a walker within 1 day of surgery. Return home occurs at 1–3 days. Driving resumes at 3–6 weeks (longer for left hip in manual transmission vehicles). Return to most activities at 6–12 weeks; full recovery at 3–6 months with complete physical therapy engagement.
Q3. What is avascular necrosis of the hip?
A: Osteonecrosis (avascular necrosis) of the femoral head — disruption of blood supply causing bone death and eventual collapse of the hip joint surface. Risk factors include corticosteroid use, excessive alcohol, sickle cell disease, and trauma. Early stages are managed conservatively; late-stage collapse often requires hip replacement.
Q4. Can hip pain radiate down the leg?
A: Yes. Hip joint pathology can refer pain to the thigh. Lumbar spine pathology (sciatica, hip flexor tightness) can cause pain perceived in the hip and thigh. Distinguishing true hip joint pain from referred pain requires careful clinical examination and sometimes diagnostic injection to confirm the pain source.
Q5. At what age does hip replacement become necessary?
A: Hip replacement is not age-dependent — it is symptom- and function-dependent. The indication is severe pain not controlled by optimal conservative management that significantly limits daily function. Modern implants last 15–20+ years, making it appropriate for both younger and older adults when clinically indicated.